

The Triglyceride Trap:** When “Not That High” Becomes “Why Is He in the ICU?”
Reviewing Mach et al. “2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias.” *Eur Heart J*, 2025.

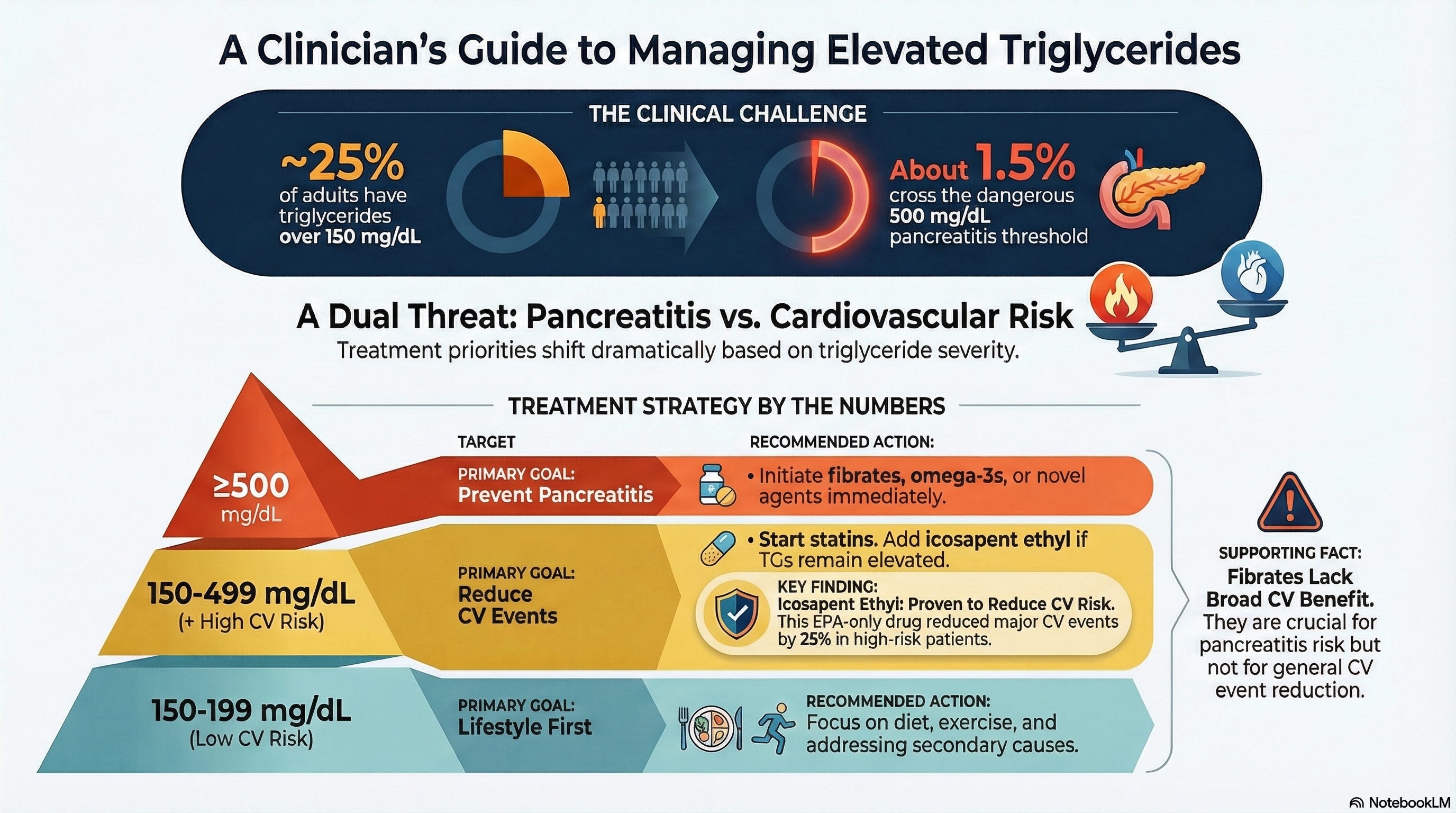
Clinical Focus Question: In adults with persistent hypertriglyceridemia, when does lowering triglycerides mainly prevent pancreatitis versus meaningfully reduce ASCVD events—and what does the ESC/EAS 2025 update actually push clinicians to do differently at the bedside?
Why this matters bedside
The patient with triglycerides in the 200s–400s is the one who quietly eats visit time: not sick enough to trigger urgency, not normal enough to ignore, and often on a growing pile of meds already.
The 2025 ESC/EAS focused update is a useful forcing function because it makes a very specific move in that “gray zone”: it says **high-dose icosapent ethyl (2 g twice daily)** should be considered *with a statin* in high-risk/very-high-risk patients when fasting triglycerides are 135–499 mg/dL to reduce cardiovascular events.
At the other extreme—the “please don’t let this person get pancreatitis again” end of the spectrum—the same update adds a recommendation to consider volanesorsen for familial chylomicronemia syndrome (FCS) with severe hypertriglyceridemia (>750 mg/dL) to lower triglycerides and reduce pancreatitis risk.
Meet Mr. J
Mr. J is 52, has type 2 diabetes, obesity, and a statin on board; his LDL-C is “fine,” but fasting triglycerides keep hovering around 320 mg/dL despite honest attempts at diet changes and improved glucose control.
He’s not coming in asking for triglyceride optimization—he’s asking whether he’s “safe,” whether he’s going to have a heart attack like his older brother, and whether another prescription is worth the cost and side effects.
This is the exact clinical intersection where ESC/EAS 2025 tries to clarify the next step: triglycerides aren’t just a lab nuisance; in the right risk category, they become a trigger for targeted therapy (icosapent ethyl) aimed at *events*, not just prettier numbers.
Lets Dive Into ESC/EAS 2025
This is not a randomized trial; it’s a focused guideline update (published August 2025) that updates recommendations from the 2019 ESC/EAS dyslipidaemia guideline based on evidence accrued through March 31, 2025.
The hypertriglyceridemia “new recommendations” slide is blunt: high-dose icosapent ethyl (2 × 2 g/day) *should be considered* in combination with a statin for high- or very-high-risk patients when fasting triglycerides are 135–499 mg/dL, specifically to reduce cardiovascular events (Class IIa, Level B).
In plain bedside english: if the patient’s risk is high enough and triglycerides sit in that 135–499 mg/dL range despite statin therapy, ESC/EAS is giving permission—almost a nudge—to treat beyond LDL-C, using the one omega-3 strategy that has consistently been framed as event-reducing in this space (EPA-only, high dose).
“For high- or very-high-risk patients on statins with fasting triglycerides 135–499 mg/dL, ESC/EAS 2025 says to consider icosapent ethyl 2 g twice daily to reduce cardiovascular events—not to ‘fix the lab.’”
What the guideline does *not* say (and why that matters)
The ESC/EAS 2025 update does not present triglyceride lowering as a universal goal in everyone with mild-to-moderate elevations; the recommendation is explicitly tied to *risk category* and *concomitant statin therapy*.
That framing matters because it keeps clinicians from reflexively adding therapies to every patient with triglycerides of 180 mg/dL, while still acknowledging that for the right patient, triglycerides are a signal of remnant risk worth addressing.
It also implicitly reinforces that lifestyle and secondary-cause workup are the foundation, since pharmacologic escalation is positioned as “should be considered” rather than “must be done.”
Ancillary evidence (to support, not steal the show)
If the ESC/EAS update is the “what,” REDUCE-IT has historically been the “why” clinicians remember: it’s the trial most commonly cited when guidelines recommend high-dose EPA (icosapent ethyl) on top of statins in patients with elevated triglycerides and high cardiovascular risk.[1]
“In severe hypertriglyceridemia, the story isn’t cardiovascular prevention—it’s pancreatitis prevention, and new apoC-III therapies are forcing us to think beyond fibrates.”[2]
On the pancreatitis-prevention side, new apoC-III–targeting therapies are pushing the field because they don’t just shave triglycerides—they may move a large proportion of patients below the classic pancreatitis risk thresholds.[2]
In the CORE-TIMI severe hypertriglyceridemia program (CORE-TIMI 72a and CORE2-TIMI 72b), olezarsen substantially lowered triglycerides and was associated with a markedly lower pancreatitis event rate versus placebo, with hepatic fat fraction increases raising real-world monitoring questions.[3][2]
How ESC/EAS 2025 changes the conversation
For triglycerides 135–499 mg/dL, ESC/EAS 2025 essentially asks two questions before adding icosapent ethyl: (1) is the patient high or very high risk, and (2) are they already on statin therapy (or at least have statin therapy as the backbone)?
If both answers are “yes,” the guideline-supported move is icosapent ethyl 2 g twice daily *in addition* to the statin, with the explicit goal of reducing cardiovascular events (Class IIa, Level B).
“ESC/EAS 2025 doesn’t ask you to chase triglycerides in everyone—it asks you to treat risk, and to consider high-dose EPA *only* in high/very-high-risk patients already on statins.”
For the patient, the translation is: “This isn’t about chasing a lab number; it’s about lowering the chance of the next heart attack or stroke in someone whose overall risk is already high.”
Critical appraisal and limitations (of acting on this)
A focused update gives recommendations, not patient-level guarantees—so the bedside reality is still selection, adherence, and cost, plus the uncomfortable truth that triglycerides often track with metabolic health you can’t fix with a prescription alone.
Even in the exciting severe-hypertriglyceridemia drug space, the olezarsen program flagged potential trade-offs (hepatic fat fraction increases and small HbA1c increases), which is a reminder that dramatic triglyceride lowering can come with new monitoring burdens.[2]
Unanswered questions that remain clinically annoying: how best to prioritize icosapent ethyl versus other add-ons in polypharmacy-heavy patients, whether benefits generalize cleanly across diverse real-world diets and adherence patterns, and how to sequence emerging apoC-III/ANGPTL3-targeting agents once outcome trials mature.[2]
If you only read the headline, you might think ESC/EAS 2025 “tells us to treat triglycerides.” Once you look under the hood, it really tells us to treat **risk**—and to use triglycerides as a lever only when the patient is already high/very-high risk and already on a statin.
Practical guidance (busy clinic version)
Step 1: Confirm the number** (fasting if needed) and look for secondary causes (alcohol, uncontrolled diabetes, hypothyroidism, meds) before adding therapy.
Step 2: Risk-category first, not triglyceride-first**: if the patient is high or very high ASCVD risk, ESC/EAS 2025 supports considering icosapent ethyl when fasting triglycerides are 135–499 mg/dL despite statins.
Step 3: Say the goal out loud**: “This add-on is for event reduction,” not “because your triglycerides annoy me.”
Step 4: Severe levels are a different emergency**: in very high triglycerides—especially with pancreatitis history—think pancreatitis prevention strategy and recognize that FCS is its own category with specific therapies discussed in the guideline update (e.g., volanesorsen for FCS >750 mg/dL).
Candid implementation reflection
In practice, the hardest part isn’t knowing that icosapent ethyl is “reasonable”—it’s deciding when the patient’s risk is high enough that adding a twice-daily medication is a net win rather than just another adherence failure waiting to happen.
ESC/EAS 2025 helps by narrowing the lane: high/very-high risk, on statin, fasting triglycerides 135–499 mg/dL—then consider high-dose EPA.
For severe hypertriglyceridemia, the emerging apoC-III therapy data are compelling, but the hepatic fat signal (and the reality of access) means this is not yet a “prescribe and forget” category.[2]
Guidelines search and summary (ESC/EAS 2025 focus)
Searched: ESC Clinical Practice Guidelines page for the “Focused Update on Dyslipidaemias,” plus the official ESC slide set for the 2025 focused update recommendations.[4]
Key hypertriglyceridemia recommendations located in the “New Recommendations” section include: (1) consider high-dose icosapent ethyl (2 × 2 g/day) with a statin in high/very-high-risk patients with fasting triglycerides 135–499 mg/dL to reduce cardiovascular events (Class IIa, Level B), and (2) consider volanesorsen 300 mg/week in severe hypertriglyceridemia (>750 mg/dL) due to FCS to lower triglycerides and reduce pancreatitis risk (Class IIa, Level B).
Challenge to the Lounge
When triglycerides are 200–400 mg/dL in a patient already on a statin: what’s the tipping point that makes you actually prescribe icosapent ethyl—ASCVD history, CAC score, diabetes duration, something else?
References
1. Mach F, Koskinas KC, Roeters van Lennep J, et al. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias. *Eur Heart J*. Published online August 29, 2025. doi:10.1093/eurheartj/ehaf190.
2. TCTMD. Olezarsen cuts triglycerides, pancreatitis risk in severe hypertriglyceridemia. Published November 13, 2025. Accessed December 29, 2025. https://www.tctmd.com/news/olezarsen-cuts-triglycerides-pancreatitis-risk-severe-hypertriglyceridemia.[2]
3. American College of Cardiology. Olezarsen for managing severe hypertriglyceridemia and pancreatitis risk (CORE-TIMI 72a and CORE2-TIMI 72b). Published November 19, 2025. Accessed December 29, 2025. https://www.acc.org/latest-in-cardiology/clinical-trials/2025/11/20/22/00/core-timi.[3]
4. TCTMD. ESC/EAS stress early LDL-lowering in select high-risk patients (includes hypertriglyceridemia recommendation context). Published September 10, 2025. Accessed December 29, 2025. https://www.tctmd.com/news/esceas-stress-early-ldl-lowering-select-high-risk-patients.[1]