

When Help Is Too Far Away: Practicing Inside a Mental Health Provider Shortage
Reviewing Kim et al, Psychiatr Serv, 2025; Lombardi et al, J Behav Health Serv Res, 2024; Counseling Today, 2023



6 minute read
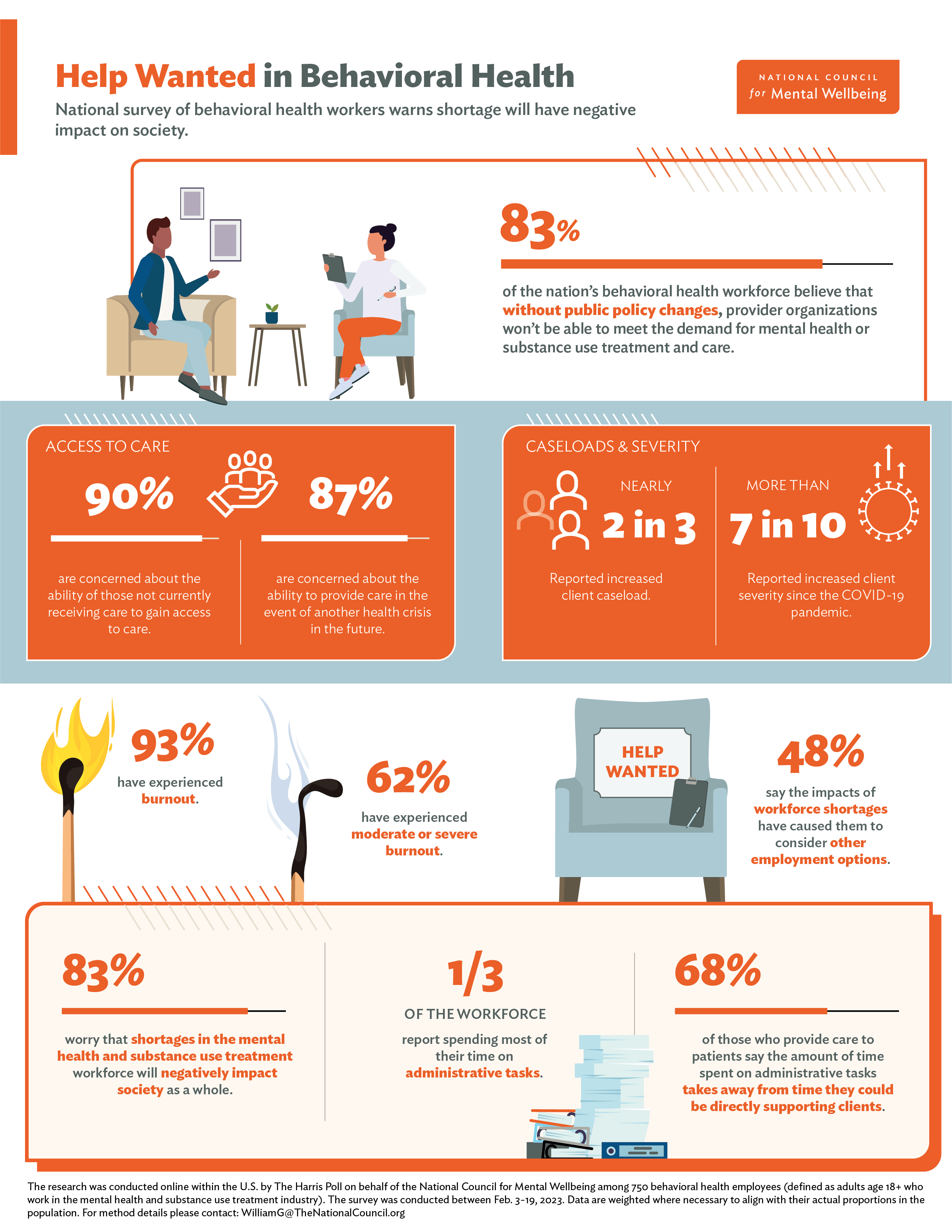
Nearly half of my patients live in mental health workforce shortage areas, where high caseloads, geographic maldistribution, and payment barriers turn “please get therapy” into weeks or months of waiting—especially for rural, disadvantaged, and minority communities.[1-3]
When I look at the workforce data, counselors are more likely than psychologists or social workers to be physically present in high-need neighborhoods, but reimbursement rules and insurance participation still determine whether that presence translates into actual access.
The Referral That Goes Nowhere
I’ve lost count of how many times I’ve handed a patient a list of therapists, only to have them return weeks later with the same problem and zero appointments scheduled. Ten calls, no callbacks. Six-month waitlists. Practices that stopped accepting their insurance. It’s a pattern I see constantly.
Federal data estimate that about 47% of the U.S. population—roughly half the country—lives in a designated mental health workforce shortage area. That’s not just a statistic; it means my discharge plans often land in communities where waitlists stretch for months, agencies are chronically understaffed, and school counselors or primary care teams absorb way more risk than they should.[2][3]

What’s Actually Driving This
Look, this shortage isn’t some overnight phenomenon triggered by the pandemic. It’s the predictable result of a system that’s treated mental health as optional for decades. When I look at the workforce data alongside what I see clinically, a few things jump out.[3][2]
**Chronic underpayment.** Mental health gets reimbursed like it’s an optional add-on to “real” medicine. Medicaid rates for behavioral health consistently trail Medicare and commercial plans—and psychiatric services often see particularly low rates. So when Medicaid expansion brought more insured patients, psychiatrists’ acceptance of Medicaid didn’t meaningfully budge. Honestly, if I were a new graduate deciding where to practice, those fee schedules would factor heavily.[2][3]
**Stagnant pay and poor retention.** Colleagues in counseling education tell me that in some community agencies, starting wages for master’s-level therapists were $18/hour in 2009—and still $18/hour in 2017. Same hourly rate, higher living costs, more student debt, less guaranteed supervision. I mean, I get why new clinicians choose private practice, telehealth-only panels, or just leave the field altogether.[3]
**Unsustainable caseloads.** In parts of rural western Colorado, one school-based clinician is responsible for roughly 470 people. When that’s your denominator, every new referral feels like a crisis you may not have capacity to manage. Similar patterns show up across rural and frontier areas—long distances, limited backup, and the constant worry that you’re one resignation away from losing the last therapist in town.[1][3]
**Geographic maldistribution.** A national analysis using the Area Deprivation Index found roughly 351 behavioral health clinicians per 100k people in the least disadvantaged communities, but only about 267 per 100k in the most disadvantaged areas. Psychologists and social workers were especially scarce in high-need neighborhoods; counselors were somewhat more common there—but until very recently, many counselors couldn’t bill Medicare at all. So even when a clinician is physically present in a high-need zip code, payment rules may prevent my Medicare or Medicaid patients from seeing them.[1]
Who Gets Left Behind
In clinic, the shortage doesn’t show up as “lack of FTEs.” It shows up as patients who get stuck. Older adults with depression and chronic disease living an hour from the nearest psychologist. Adolescents with escalating self-harm whose families have insurance but can’t find a child therapist taking new patients within a reasonable drive. They cycle through the ED, get admitted, and are discharged with recommendations for outpatient therapy that simply doesn’t exist locally.[3]
The data back this up: youth and adults in Mental Health Professional Shortage Areas have higher suicide rates, and that gap widened between 2010 and 2018. Rural communities and socially disadvantaged neighborhoods are more likely to have zero behavioral health clinicians nearby—and when clinicians are present, they’re stretched thin.[2][1]
Layer in race and culture, and the picture gets sharper. Black clinicians make up a small slice of the mental health workforce nationally, and Black patients who want a racially concordant therapist often run into even longer waitlists or travel distances. Given what we know about concordance and engagement, that’s not a small detail—it’s another way the shortage amplifies existing inequities.[2][3]
Coverage Doesn’t Equal Access
Here’s something that caught me off guard: expanding insurance coverage alone hasn’t been enough to “fix” access. A California analysis of adults with serious psychological distress (SPD) found that uninsured rates dropped under the ACA in both shortage and non-shortage areas, but changes in actual mental health service use were modest and didn’t differ by shortage status. Specialty mental health visits did rise in non-shortage areas, but not enough to close gaps.[2]
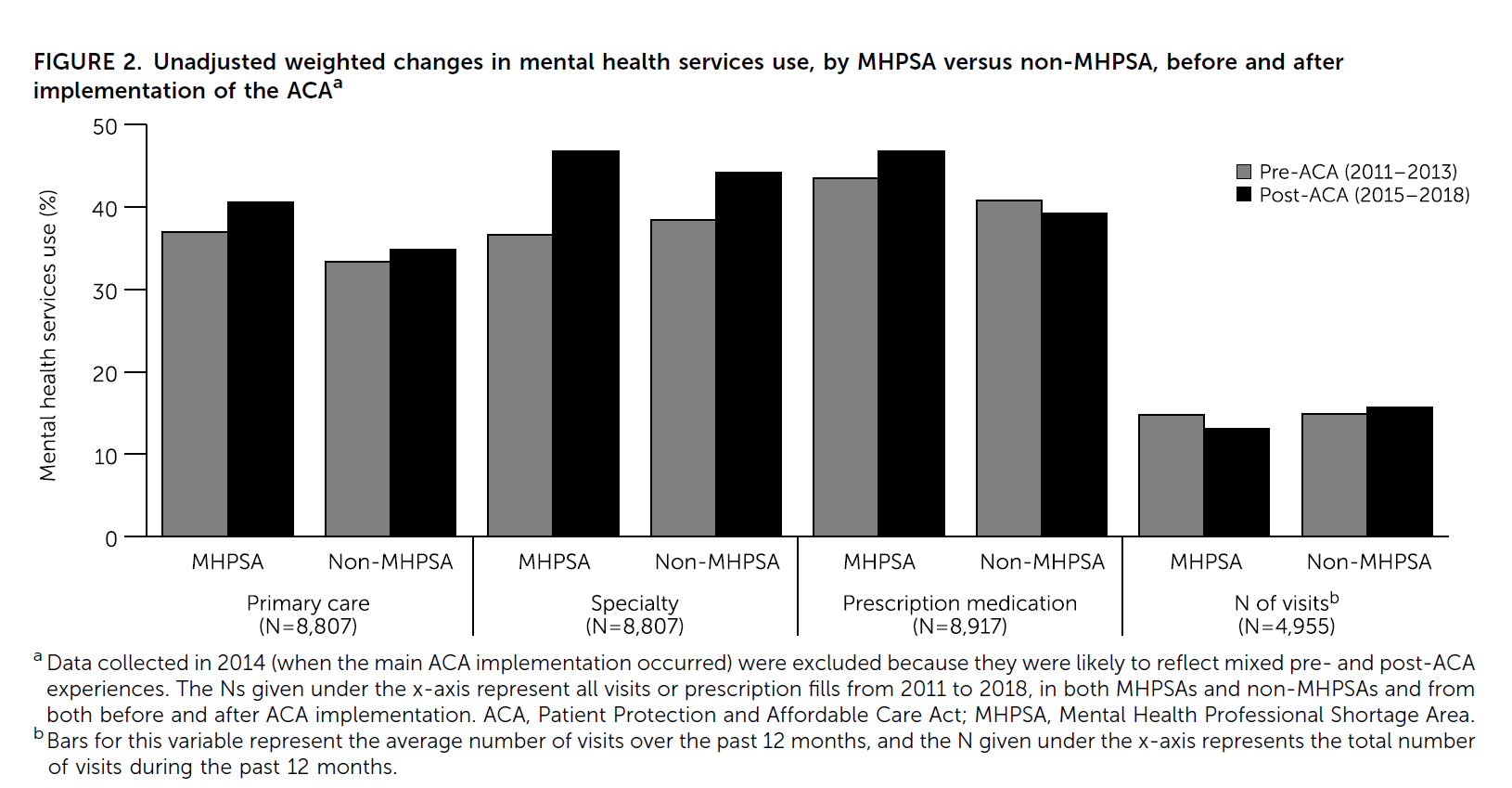
That’s consistent with what I see. Insurance cards are necessary but not sufficient. If a patient has a plan that nominally covers therapy, but there are no local clinicians taking that plan—or the nearest one has a three-month wait—the effect is the same as being uninsured.
The distinction here is between coverage and capacity. Coverage changes who could be seen. Capacity determines who actually gets seen, when, and by whom. Without deliberate workforce and payment reform, coverage expansions alone won’t meaningfully shorten the line.[1][2]
What I Do Differently Now
I can’t solve the workforce shortage from my clinic room, but I’ve adjusted how I practice in light of it—and I think that’s where these data become clinically useful.
When I’m about to say, “Just get a therapist,” I pause and ask about geography, transportation, language, and prior attempts to find care. For someone in a rural, high-disadvantage area, I assume access will be constrained and build more structured follow-up into my own plan.[3][1]
I lean harder on integrated models—embedding brief behavioral interventions in primary care, using telehealth options that are genuinely accessible, and collaborating with school-based or community counselors even when they’re outside my usual referral network.[1][3]
And I support policy changes that reflect where clinicians actually are. Expanding reimbursement to licensed counselors and marriage/family therapists—especially in Medicare and Medicaid—taps into a workforce that’s already overrepresented in high-need communities. Loan repayment, rural stipends, telehealth-friendly regulations—these aren’t abstractions anymore; they’re tools that may change whether my next patient finds someone to call back.[1]
Clinical Bottom Line
**Treat referral access as a clinical variable:** When patients can’t access therapy, outcomes worsen. Factor waitlist times and geographic barriers into your management plan.[3][2]
**Push for payment parity and billing reform:** Support policies that expand reimbursement for all licensed clinicians and raise Medicaid rates to match the complexity of behavioral health care.[2][1]
**Lean on telehealth and integrated care:** These approaches extend reach and reduce burnout, especially in underserved areas. Push for policy that sustains them beyond the pandemic.[3][1]
My diagnostic reasoning and treatment planning are only as good as the system patients move through after they leave the room.[1-3] A mental health provider shortage isn’t just a workforce statistic; it’s the quiet reality that shapes whether my “best practice” plan turns into actual care—or into another patient asking for a refill because there was nowhere else to go.
References
1. Kim LH, Hodgkin D, Larson MJ, Doonan M. Changes in mental health services use under the ACA in one state: role of mental health provider shortages. Psychiatr Serv. 2025;76(2):149-156. doi:10.1176/appi.ps.20230628
2. Lombardi B, de Saxe Zerden L, Jensen T, Galloway E, Gaiser M. Behavioral health workforce distribution in socially disadvantaged communities. J Behav Health Serv Res. 2024;51:168-179. doi:10.1007/s11414-024-09897-0
3. A closer look at the mental health provider shortage. Counseling Today. May 2023. Accessed January 1, 2026. https://ct.counseling.org/2023/05/a-closer-look-at-the-mental-health-provider-shortage