

Nerve Blocks, Not Narcotics: The 2025 AHS Guideline Rewrites the ED Migraine Playbook


The Bottom Line
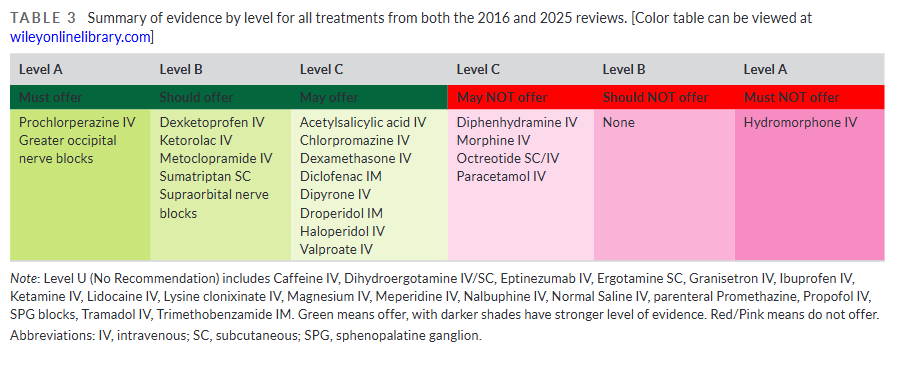
Current standard of care: The 2016 AHS guideline recommended IV prochlorperazine, IV metoclopramide, and SC sumatriptan as Level B treatments for acute migraine in the ED. Opioids landed at Level C, meaning clinicians could avoid them. Even so, opioids still showed up in about 28% of ED migraine visits as late as 2018, and only 37% of patients left the ED headache-free.
What this evidence adds: Two treatments now move to Level A, which means must offer: IV prochlorperazine and greater occipital nerve block, or GONB. Hydromorphone moves to Level A in the opposite direction: must not offer. That is new territory for the AHS. Dexketoprofen IV and ketorolac IV also move up from Level C to Level B.
The fine print: The panel did not perform formal meta-analyses because the trials were too different to pool. A lot of the studies were small, often under 100 patients, and their outcome windows ranged from 30 minutes to 2 hours. That makes side-by-side comparison messier than the recommendation table suggests. The eptinezumab data also come from an outpatient population, not the ED.
The 2 AM Migraine That Won’t Break
A 34-year-old woman rolls into the ED at 2 AM with her head under a blanket and a basin in her lap. She is vomiting, photophobic, and 14 hours into a migraine that already blew through her home sumatriptan. The nurse asks what to hang.
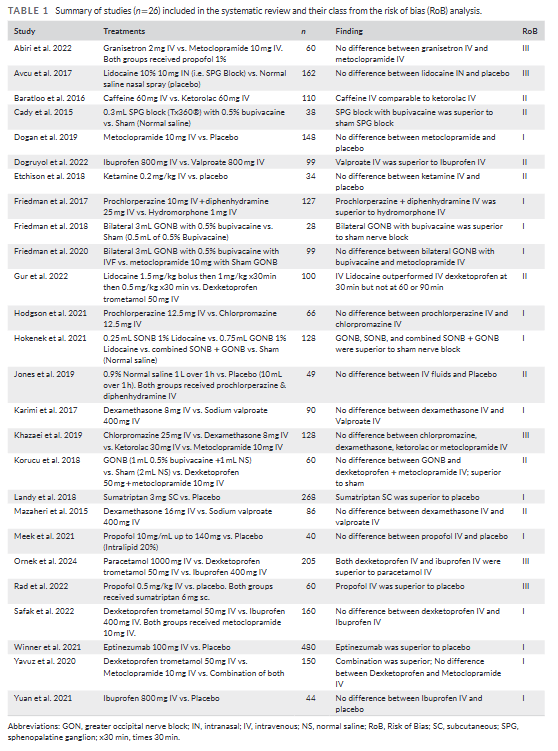
For a long time, the answer was some version of Compazine and Toradol. The 2025 AHS update still points toward that lane, but it is more explicit now. The panel reviewed 26 new randomized trials with more than 3,000 participants and layered them onto the 2016 evidence base. For the first time, it also issues Level A recommendations in this setting.
Robblee and colleagues limited the review to injectable treatments for adults in the ED with ICHD-diagnosed migraine: IV, IM, SC, and nerve blocks. They graded the studies with the AAN risk-of-bias framework, then converted those ratings into recommendation levels from A down to U.
Prochlorperazine Gets Its Promotion
The clearest change is prochlorperazine. IV prochlorperazine moves from Level B to Level A.
That shift mostly rests on Friedman et al. 2017, a 127-patient trial comparing prochlorperazine 10 mg IV plus diphenhydramine 25 mg IV with hydromorphone 1 mg IV. Sustained headache relief at 48 hours was 60% with prochlorperazine and 31% with hydromorphone. The number needed to treat was 4. The trial stopped early because the benefit was large enough that the data monitoring committee called it.
That same trial drags hydromorphone down to Level A must not offer. That wording is a big deal. Patients in the hydromorphone group had more adverse effects, needed more rescue medication, stayed longer in the ED, and returned more often. The guideline leaves a narrow exception for patients with no real alternatives, a stable prior opioid response, and low dependence risk.
Still, this part deserves a raised eyebrow. The hydromorphone downgrade leans heavily on one Class I trial. It is a good trial, and it lines up with the older sense that opioids were a poor choice here anyway. But the strength of the recommendation is broader than the size of the direct evidence base.
The Nerve Block Surprise
GONB did not even get a formal grade in the 2016 guideline. Now it lands at Level A.
That is the most surprising part of the update. The support comes from three Class I studies and one Class II study. Two sham-controlled Class I trials found that GONB with bupivacaine or lidocaine beat sham. A third Class I trial found that it performed about as well as IV metoclopramide.
But that third study, Friedman 2020, is not quite as clean as the headline suggests. Metoclopramide actually leaned a little better than GONB, with a between-group difference of negative 1.1 and a 95% confidence interval from negative 2.3 to 0.1. The interval barely crosses zero, so this was close. Then there is the operator issue. When the clinician had done at least seven prior nerve blocks, every patient in that subgroup got more than 50% pain relief. Less experienced operators did worse.
That matters. A recommendation level cannot standardize technique. So the real-world version of “must offer GONB” probably depends on whether someone in the department actually knows how to do it.
Supraorbital nerve block lands at Level B. It beat sham in the Hokenek trial, but it did not do as well as GONB. The guideline suggests combining the two when that is feasible.
The NSAID Shuffle
Dexketoprofen IV, which is not available in the United States, moves from Level C to Level B. The data behind it are fairly steady. It beats placebo and looks roughly comparable to metoclopramide.
The most interesting dexketoprofen study is probably Yavuz et al. In that 150-patient trial, dexketoprofen 50 mg IV plus metoclopramide 10 mg IV worked better at 30 minutes than either drug alone. That is one of the few places in the guideline where combination therapy gets a real signal rather than just a theoretical appeal.
Ketorolac IV also moves up from Level C to Level B. Most of the important evidence is older, but the newer Class II and III studies do not really argue against it. So the promotion feels more like a steady accumulation of support than a dramatic turn.
IV ibuprofen gets Level U, which is the panel’s way of saying the evidence still does not settle the question. One Class I placebo-controlled trial found no significant difference from placebo. Another found results similar to dexketoprofen. That is not enough to hang a recommendation on.
IV paracetamol, or acetaminophen, loses ground. It drops from Level C may offer to Level C may not offer. Between the older negative placebo-controlled trial and later studies showing no clear advantage over active comparators, the guideline seems to have lost patience with it.
The Eptinezumab Question
Eptinezumab is where the data and the real world start pulling apart.
In the Winner et al. Class I trial, 480 patients were randomized, and eptinezumab beat placebo for acute treatment. Headache freedom at 2 hours was 23.5% versus 12.0%. That is statistically solid and clinically real. But the trial population was so selective that the result does not travel cleanly into the ED.
So the guideline splits the recommendation. Eptinezumab gets Level B for patients who match the trial population, but Level U for general ED use. That split feels fair. These were outpatient infusion-center patients with 4 to 15 monthly migraine days, prior triptan use, and a treated attack that started after at least 24 headache-free hours. That is not the usual ED patient who has been hurting all day and already failed home treatment.
Then there are the practical barriers. Cost matters. Prior authorization matters. The pregnancy washout period matters. So even though the absolute headache-freedom benefit was 11.6%, this still feels more like an interesting signal than something most EDs can build around right now.
What Didn’t Move
Metoclopramide stays at Level B.
At first glance that may look odd, because the Dogan trial found no significant difference from placebo at 30 minutes. But 30 minutes is earlier than the usual assessment point in most metoclopramide studies, and the secondary outcomes still leaned its way. Once that trial gets added to the earlier Class I data, the guideline’s decision to leave metoclopramide at Level B makes sense.
Propofol did not hold up as well. Earlier lower-quality studies had made it look promising, but a later Class I trial found no difference from placebo. The blinding issue also hangs over the whole question. People usually know when propofol has been given, which makes “masked” comparison harder to believe.
Clinical Impact
For the patient already in the ED with a diagnosed migraine, no obvious contraindication to dopamine antagonists or local anesthetics, and a reason to use parenteral therapy, the order set is clearer than it used to be. Start with IV prochlorperazine. Consider bilateral GONB if someone available is actually good at it. Add dexamethasone to reduce recurrence. Use ketorolac or dexketoprofen as adjuncts when NSAIDs fit.
The patient who clearly loses in this update is the one getting IV hydromorphone. The guideline does not hedge. The exception is so narrow that it will apply only rarely in actual practice. What practice that is, I still don’t know.
The bigger implementation question is GONB. A Level A recommendation sounds strong on paper, but it does not matter much if nobody on shift has done the procedure more than once or twice. That is the part I keep coming back to. This update may change migraine care in departments that train for the block. In departments that do not, prochlorperazine will remain the backbone, just with stronger backing than before.